
“Sacred cows make the best hamburgers.”
- Mark Twain
Death is practically a taboo topic in modern society. We are very poor explorers of life’s greatest unknown. Maybe you can change that.
The COVID-19 pandemic made the world pay more attention to one of the most neglected aspects of death: the things we require to die well. Until vaccines became available, the best way to “flatten the curve” was large-scale physical distancing. That had the unintended consequence of making death much more painful than it already is: family separation, the prospect of dying alone, the lack of final goodbyes, the coldness of virtual funerals, the mass graves.
In hindsight, our plans for dealing with a pandemic were weak. Our plans for dignifying the deaths caused by a pandemic were non-existent.
A century of medical breakthroughs has improved our lives. Has it also wrecked our relationship with death? If so, now may be your best opportunity in several generations to help us fix that relationship. But doing so will demand feats of original thinking and brave conversation.
The journey promises to be rewarding, for self and society. “In learning how to die we might also be taught how to live,” writes the philosopher Simon Chritchley.
Is he right? Some of us will have to risk the journey to find out.
Are we avoiding death?
20th century medical developments are a marvel. Penicillin has made surgeries safer and made once-deadly diseases harmless. Breast cancer mortality has dropped by 34% the last 50-odd years. Infant mortality has dropped by almost 90% since the industrial revolution. For those living in wealthy advanced economies, death has become a rare occurrence. It has become abnormal.
Has that hurt our relationship with death?
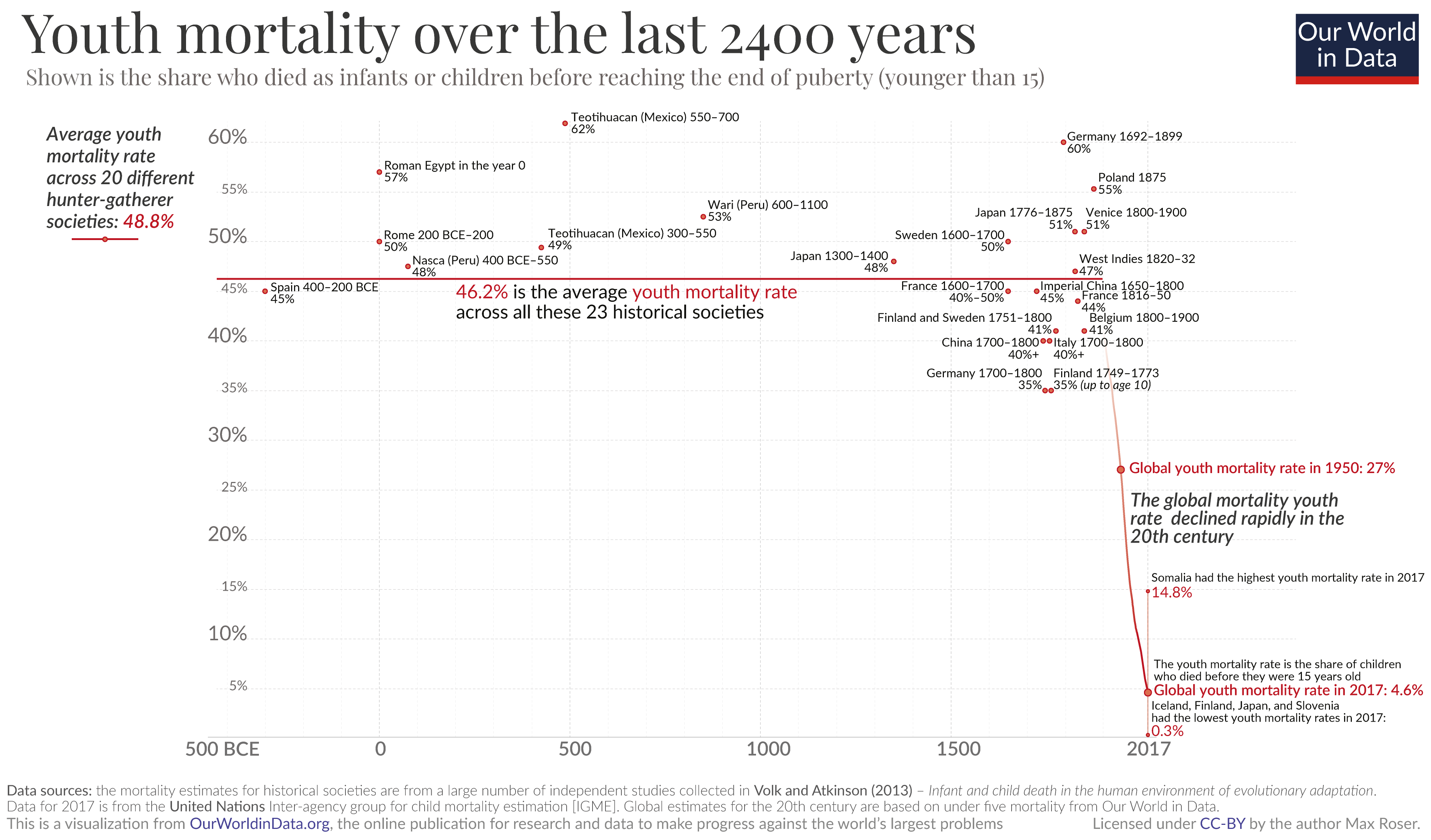
For most of human history, people grew up around death. Almost half of children would die before the age of fifteen. Infections or viruses claimed lives with punishing regularity. Life and death were always close: women giving birth in living rooms, family members dying on farms or when hunting.
Today, life and death stand farther apart. Childbirth often takes place in a hospital, with little or no family watching (a trend that COVID accelerated). Death, and the journey leading up to it, now seldom happens at home. Instead, older people are often placed in care homes to be closer to professional caregivers – and may die surrounded by strangers as a result.
Death has gone from an experience that society strives to defer – through vaccines, antibiotics, safer work conditions – to an experience that society strives to eliminate.
We rarely see death, let alone a good death. Absent that experience, are we are becoming hostile to the whole idea? A Pew Research poll from 2013 showed that with every passing year, fewer people believe that it is okay to sometimes allow a patient to die. Should a doctor always do everything in their power to save a patient? Twice as many people agreed with that statement in 2013 than agreed with it in 1990.
The one thing that is guaranteed to happen to everyone has become unnatural.
Talking about the end of one’s life is a taboo topic. The current way of approaching the question of death echoes the abstinence-only approach to sex education: Death, and talking about it, should be avoided. Not talking about sex doesn’t stop people from having sex. Not talking about death will not stop people from dying, either.
What is a good death?
An under-challenged assumption is that the way to make life better is to make life longer. Historically, that made a lot of sense. A major obstacle to living a fulfilling life was the risk of having it cut short. In the 21st century, this is less of an obstacle. With life expectancies in the 80s in many advanced economies, is that now enough time to live a fulfilling life? Does this one-dimensional life-line still make sense?
.png)
Ask elders how they feel about dying, and many do not fear death. Instead, they fear the incontinence, the loneliness, the deteriorating functionality of mind and body. (The ageing of society, and the growing share of elderly people in society, means the number of people living with dementia globally will more than double between now and 2050.) The nuance for them is delicate: it is not the absence of life that worries many elders, but living without dignity, or living with pain. Does that count as “being alive” at all?
Medicine can extend life. Does it also extend dying?
A good death does not by definition have to be at the end of a long life, nor does the presence of life guarantee a situation that is better than death. Our picture needs a second dimension, quality, to capture this range of possible experiences.

On screen this picture looks innocent enough; in real life it’s highly controversial. The picture suggests these axes are treated equal. They’re not. The societal urge to keep people alive at all costs is so strong that many who have made written wills asking for assisted suicide once their dementia reaches a certain stage are denied that choice. Is that exactly right or terribly wrong?
These are hard cases. They are only going to get harder.
In the Netherlands in 2019, a 17-year-old girl with severe depression and post-traumatic stress had her request for medical euthanasia turned down. She still died, but only after purposefully starving herself to death. In 2018, another young woman, this time 29 years old, had her request accepted due to feeling “chronically suicidal.” Both these young people judged an early death on their own terms to be more humane and reasonable than one in the distant future, despite both being physically healthy. Their decisions run sharply contrary to today’s prevailing norms.
How do you react to them?
We all want control over our own life’s journey. In the end, might your control be overridden? If you intend to challenge prevailing social norms surrounding death, will you face well-intentioned and loving people who are convinced that death is inherently bad, that something is better than nothing, that hope springs eternal, or that the new normal of medical life-support is better than dying on your own terms?
Is death the end?
“To leave a legacy” is a common ambition. Often, the urgent feeling behind this phrase is to do big enough things while we’re living so that people will still remember us when we’re gone.
But many of our own life’s biggest consequences may not be revealed until long after we’re gone.
Van Gogh famously only sold one painting in his lifetime, yet became one of the most influential painters in European history after his death. Das Kapital by Karl Marx was published more than 130 years ago, and it ranks in the Top 20 of today’s most cited books in social science. Michel Foucault, dead for almost forty years, has been cited over 80,000 times per year, every year, since 2016.
The pathways to posthumous impact are many and mysterious. Lucy, the name given to our 3.2-million-year-old female ancestor in Ethiopia, might be the most famous archaeological discovery in history. Her bones taught us that the ability to walk upright predated the large brains seen in modern humans. By some estimates, there are more people alive today researching the ancient city of Babylon than actually lived in Babylon at its height roughly 4,000 years ago. Though long dead, those people continue to teach us. Anne Frank’s diary might be the most famous piece of Holocaust-related literature, despite Ms Frank explicitly using it for thoughts she had “never been able to confide in anyone” else.
In a more immediate way, organ donors have a transforming impact on the lives of those persons who receive their organs. A single donor can save up to eight lives. Relatives of organ donors often take solace in the fact that their grief gives someone else a renewed chance at life. People involved in the process often feel as if the donor lives on.
Death may be the end of our lives, but it may not be the end of our impact on the world.
“Is there an afterlife?” This question concerns the continuation of our own consciousness, and we ask it a lot.
“Is there an aftermath?” This question concerns the continuation of our life’s consequences – and do we ask it enough?
.png)
If we had more certainty about our aftermath, would it change the culture of celebrity? Would people become less worried about accumulating followers, and more worried that chasing after them might distract us from doing something longer lasting?
If we had more certainty about the aftermath, would it change the culture of productivity? “Getting things done” is a popular mantra and hashtag (#GTD). “Leaving things unfinished” is less catchy, but it may be more important in the long run. If we look back, we can all find examples of doing things where, in hindsight, our greatest contribution was getting it started.
In a time when the strength of one's “influence” is measured moment-to-moment by the size of your digital audience, it may be harder now than at any other time in history to recognize the reality of aftermath. Nonetheless, it is real.
The things we will never live to see may be the most lasting things about all of us.
How does that change the picture?
Opportunities for action
→For individuals
We need brave new conversations about death. Can you convene them?
Our desire to prevent death, combined with our inability to do so, has led to a dearth of conversation on the topic. It’s making it very difficult for any of us to gain a richer relationship with death, because right now the dominant response to the topic is silence.
We’re very poor explorers of life’s greatest unknown.
A practical starting point is to broach the topic of “a good death.” What might a good death mean to you? What might it mean to those people whose death you expect to be an important part of your own life?
.png)
Mehreen Zaman, Alex Jadad et al reviewed the entire medical literature on good death and came away with 11 conditions that people commonly cite when asked:
- Relief from physical pain and other physical symptoms
- Effective communication and relationship with health-care providers
- Performance of cultural, religious or other spiritual rituals
- Relief from emotional distress or other forms of psychological suffering
- Autonomy with regards to treatment-related decision making
- Dying at a preferred place
- Not prolonging life unnecessarily
- Awareness of the deep significance of what is happening
- Emotional support from family and friends
- Not being a burden on anyone
- Right to terminate one’s life (if legal and cultural norms allow)
The authors point out: only three of these 11 conditions (in bold) require medical expertise or infrastructure.
"The remaining conditions reflect the need to reimagine ways in which the role of medicine could be downplayed, or other available resources diverted to enable those who are dying to experience their desired and expected levels of psychological, spiritual, relational, communicational, and practical support…"
In other words, it’s not up to the medical community to define or ensure a good death. It’s up to you.
→For society
In public, the big conversations about death fix on the question of whether to die and who gets to decide it.
How to die is a missing conversation — despite the fact that so much of how we die is socially constructed. It’s a product of the rituals and dramas we take part in with other people. To change our present relationship with death, we’d need to change it together.
Humanity is rich with different death rituals. Seeing how other societies do death can help you spot the presumptions within your own world that you might want to challenge.
Take the Toraja people of Indonesia, for example. For most of the world’s population, death rituals emphasize solemnity and finality. But the Toraja emphasize the opposite — celebration and new beginnings.
They can wait weeks or even months to bury their dead, and the deceased are still fed and given water – they are, according to custom, not yet dead. Funerals are enormous, involving the whole village, and at regular intervals in later years villagers dig up the bodies (in a ceremony called ma’nene’) to converse with ancestors and dress them in new clothes – even sunglasses. For the Toraja, death is tragic but your funeral is the most important day of your life — the beginning of a new journey for your soul.
The Toraja challenge the notion that “living” or “dead” is an on/off condition, like black and white. Should we rethink that presumption too? As medical technology creates new shades of gray, do we need to bring new words into our language so we can have better conversations about the more nuanced journey that death has now become?
For many reasons — psychological, empathetic, economic, moral — we need people to break the social taboo surrounding death so we can renew its meaning in a changing world.
Can you get us started?
.svg)








{kind=link}